Illustration by Tamara Rees/VIN
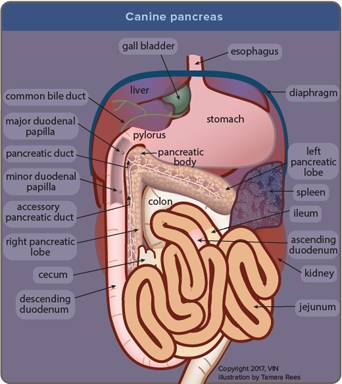
The pancreas is a small, light pink glandular organ nestled under the stomach and alongside the duodenum (upper small intestine). The endocrine pancreas is the part of the pancreas that secretes hormones involved in blood sugar regulation, such as insulin and glucagon. The exocrine pancreas produces enzymes we use to digest our food. These two parts of the pancreas are not in separate areas but instead, these two different types of pancreatic tissues are all mixed together throughout the entire pancreas.
The insulin-secreting cells are called beta cells and are bunched in groups called Islets of Langerhans, which are scattered throughout the pancreatic tissue. In some unfortunate individuals, the beta cells become tumorous and while the tumor itself can be small, its effects are large because it produces large amounts of insulin. Insulin-secreting tumors are called insulinomas.
What Happens to the Patient?
Insulin is a hormone secreted to store sugar. Normally it is secreted in response to the carbohydrates in a meal; it allows the extra sugar to be removed from the bloodstream and stored as starch and fat, thus keeping the blood sugar level within the normal range. The function of normal islets of Langerhans is tightly regulated by the body but if there is an insulin-secreting tumor, the tumor is not subject to this regulation. Insulin secretion runs wild in this situation and low blood sugar (hypoglycemia) becomes a problem.
The hypoglycemia in this situation is typically severe, most commonly resulting in seizures. Other clinical features include listlessness, twitching, trembling, apparently drunken or wobbly gait, and reduced mental awareness.
Testing
One of the first steps in evaluating any sick patient is a basic blood panel. Patients presented during a seizure are commonly screened for low blood sugar. Low blood sugar is typically recognized early in the diagnostic process, although if the blood sugar has had time to recover (if the patient has eaten or depending on what emergency medications have been given), the situation may be ambiguous. Sometimes the patient must return to the veterinarian in a fasted state to get an accurate blood sugar assessment.
Assuming hypoglycemia is confirmed, the history and basic physical examination generally rule out some obvious potential causes. Some examples of fairly obvious potential causes of hypoglycemia include:
- Toy breed puppy hypoglycemia
- Diabetic patient possibly overdosing on insulin
- Pregnant female in labor having a difficult delivery
- Extreme exercise exertion, as in hunting dog hypoglycemia
- Starvation
- Overwhelming bacterial infection
Other not-so-obvious causes of hypoglycemia include liver disease, insulinoma, and hypoadrenocorticism (Addison’s Disease). The testing that is commonly needed beyond the basic panel would include a resting cortisol level, as a normal level largely rules out hypoadrenocorticism; an ACTH stimulation test, which is the definitive test for ruling out hypoadrenocorticism; an insulin level, which must be measured at the time the patient is hypoglycemic; and possibly a bile acids liver function test if it is not clear if liver disease has been adequately ruled out by earlier findings.
What is Hypoadrenocorticism?
Hypoadrenocorticism is a deficiency in the production of cortisol, more commonly known as cortisone. Cortisol is produced by the adrenal gland and one of its functions is to raise blood sugar in anticipation of a fight or flight response. In simpler terms, if the body is anticipating exercise, such as fighting for one’s life or escaping a predator, blood sugar must be readily available for the muscles to burn. Cortisol is secreted to make that happen. (It also makes other metabolic adaptations happen but that is a story for another time.) Poor cortisol secretion can create episodes of hypoglycemia and since hypoadrenocorticism is easily treated once identified, it is important to rule it out in a hypoglycemic patient.
The Insulin Level
To be meaningful in testing for insulinoma, the insulin level must be drawn when the patient’s blood sugar level is less than 60 mg/dl (3.33 mmol/L) because the insulin level is interpreted in light of the blood sugar level. In other words, an insulin level might be within the normal range for a normal patient but might be inappropriately high in a hypoglycemic patient.
Ultrasound
Once you are confident that excessive insulin is being produced, the next step is ultrasound. There are two reasons for this:
- To locate the tumor if you are planning surgery
- To obtain a prognosis even if you are not planning surgery
If you already know too much insulin is being produced, you can be pretty sure you are tracking down an insulinoma but if a diagnosis is not clear after all the blood testing described above, ultrasound is still a good next choice. Tumors other than insulinoma can cause hypoglycemia (though they will not produce excess insulin) and ultrasound will be helpful in finding them. Most notoriously hepatoma (also known as hepatocellular carcinoma) and smooth muscle tumors (both benign and malignant and usually found in the spleen) also cause hypoglycemia. Other tumors potentially can consume enough blood sugar to create hypoglycemia and ultrasound would be an excellent way to find any.
With ultrasound, lesions in the pancreas as small as 7 mm in diameter can be identified and, in one study, it was able to locate the pancreatic tumor in 75% of cases.
CT Scan
CT scanning is not as readily available as ultrasound, but it does offer some benefits over ultrasound if it is possible to do a CT scan instead. With ultrasound, we want to confirm that there is a tumor in the pancreas and localize it so the surgeon will know where to find it without too much manipulation (which can be inflammatory to the pancreas). We also want to find any evidence of tumor spread and determine the extent of it. It turns out that CT is much more sensitive than ultrasound when it comes to getting these important answers. Basically, any information that one can get with ultrasound can be obtained by CT. The disadvantage of CT would be that it requires general anesthesia, plus CT is significantly more expensive.

An ultrasound is being conducted. Photo courtesy of DVMSound.
Staging Insulinoma
Unfortunately, most insulinomas are malignant but that does not mean they are not treatable. There is more to prognosis than just determining if a tumor is benign or malignant and this is where staging comes in. Insulinomas can be confined to the pancreas (Stage I), spread to local lymph nodes (Stage II), or spread distantly, usually to the liver (Stage III). The therapy goal is to relieve the hypoglycemia and extend the period of normal life quality. Depending on the therapy selected, it is not unusual for the Stage I and Stage II dogs to live a year and a half or more while the Stage III dogs are looking at less than 6 months. Imaging, whether you use CT or ultrasound, is going to be crucial in determining a patient's stage.
After imaging has been completed, the time has come to decide about surgery.
Treatment: Surgery
Surgically removing the insulinoma is the treatment of choice. Even if a cure cannot be achieved surgically, removing the majority of the insulin-secreting tissue should make a big difference in the patient’s quality of life so ideally this is the best direction for therapy: locating the tumor (which, as mentioned can be very small) by imaging and removing it.
That said, surgical removal of the tumor is not a simple surgery. Manipulating the tumor can cause insulin surges that result in hypoglycemia during surgery; blood sugar levels must be tightly monitored both during and after surgery. Sugar-containing IV fluids are a must. Further, manipulating the pancreas can create inflammation (pancreatitis) which is associated with pain and nausea.
Some patients have been exposed to excess insulin so long that their normal beta cells require a prolonged period to recover, and during this time the patient may require insulin injections just as a diabetic patient would.
This all sounds like a lot of risk for the treatment of a tumor with a 90 percent chance of malignancy. However, 50 percent of dogs without evidence of tumor spread at the time of surgery have had normal blood sugars for a year after partial removal of the pancreas. This is an excellent statistic and is often well worth the surgery. In one study, dogs receiving partial pancreas removal had a medial remission time of 496 days and the dogs that went on to receive medical management after signs recurred had a median survival of 1316 days. Dogs with medical management alone had a median survival of 196 days.
Treatment: Medications that Manage Hypoglycemia
Medical management is helpful for patients where surgery is not considered an option due to other risk factors, financial limitations, or a non-resectable tumor. Many months of symptom control can be achieved with diet, steroids (hormones related to cortisol that raise blood sugar), and an oral medication called diazoxide. Frequent small meals can be used to keep blood sugar in a reasonable range.
If your pet seems to be disoriented from low blood sugar, this is a potential emergency. You can give a sugar supplement like Nutrical® or Karo® syrup and then immediately seek veterinary attention. Severe hypoglycemia (low blood sugar) can be deadly if left untreated.
If or when frequent feedings prove inadequate, corticosteroids such as prednisone or dexamethasone can be used to assist in raising blood sugar. Ideally, dosing is kept as small as necessary to avoid side effects such as excessive water consumption, excessive urination, and immune suppression.
Diazoxide is a medication that promotes blood sugar elevation through a number of mechanisms including suppression of insulin secretions. An upset stomach is the most common side effect of this medication and giving the medication with food can help ease the upset. It also causes sodium retention and should not be used in heart failure patients. Concurrent liver disease may exacerbate side effects.
Other medications such as somatostatin analogs have not been as reliable in achieving results.
Treatment: Medications to Combat the Cancer
Since insulinoma is a cancer, drugs of chemotherapy can be useful in suppressing tumor spread. Such medications are commonly used after surgery has removed the bulk of the tumor or when there is evidence that the tumor has spread. One would not consider such aggressive therapy unless a biopsy has confirmed the tumor.
Streptozocin
This drug targets beta cells of the pancreas specifically. To avoid inducing kidney failure, it must be given with aggressive intravenous fluids, thus hospitalization is required for its periodic use.
Other medications that have been used or are emerging include toceranib, doxorubicin, and alloxan.
Veterinary oncologists have the most up-to-date recommendations on chemotherapy. Ask your veterinarian if a referral to an oncologist is best for you and your pet.